When taken as prescribed for HIV, pre-exposure prophylaxis (PrEP) reduces the risk of getting HIV from sex by about 99%. Now, patients have another PrEP option. For those who cannot or may not want to…
With the rise of omnichannel HCP marketing, nearly 8 in 10 physicians say digital resources are more convenient, educational, and valuable than remote rep visits*. However, in fiercely competitive markets, how can you ensure your…
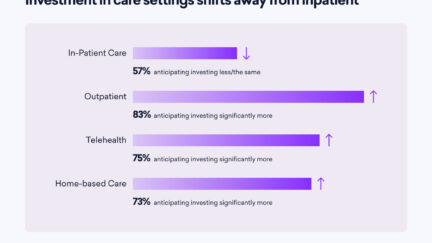
The heartbeat of the healthcare industry lies in the insights and experiences of its leaders. The most recent Sermo Barometer study from over 100 US-based healthcare leaders provides a comprehensive look at the pressing issues…
In a rapidly evolving healthcare landscape, staying ahead of the competition requires not only deep industry insights but also access to a global network of healthcare experts and decision-makers. Leveraging Sermo’s panel of healthcare experts…
Did you know that people with HIV who take antiretroviral therapy (ART) as prescribed and achieve and maintain an undetectable viral load won’t transmit HIV to their sexual partners? Treatment as prevention (TasP) is the…
The pharmaceutical marketing industry has spoken – and all signs point to omnichannel! In today’s ever-changing customer landscape and digital-first world, omnichannel is the modern marketer’s tool to deliver a seamless brand experience across channels.…
The CDC is recommending that everyone aged six months and older receive the updated Pfizer or Moderna Covid vaccines. In a recent poll of 580+ global Sermo physicians, 66% said they agree with this recommendation,…
As flu, Covid-19 & RSV infections are on the rise, the latest CDC Vaccination Trends report that almost 40% of US adults will probably or definitely not get a vaccine, and an additional 30% report…
The traditional image of a full-time physician—working long hours and available around the clock—is undergoing a transformative shift. According to a report in the Wall Street Journal, the medical profession is witnessing an increasing trend…
According to a recent report in JAMA, ER visits that are related to mental health have significantly increased among children, teenagers, and young adults. The New York Times reports, “The findings indicated an ‘urgent’ need…
The potential of AI to benefit humanity may be as great as the potential to destroy it, believe many prominent technology experts, futurists, and investors. Physicians’ opinions of AI in medicine hover in similar territory. …
By The Centers for Disease Control and Prevention (CDC) Authors: Kathleen Dooling, MD and Tara Anderson, DVM, PhD 1. The risk of developing shingles increases with age. Herpes zoster, also known as shingles, is caused…
By The Centers for Disease Control and Prevention (CDC) Author: Agam Rao, MD Agam Rao, MD is the medical officer with the Poxvirus and Rabies Branch of the U.S. Centers for Disease Control and Prevention.…